





 8 / 20
8 / 20

8 JCN supplement
2018,Vol 32, No 2
EVIDENCE-BASED PRACTICE
2011), and results of systematic
reviews that only take higher level
evidence into consideration. An
‘evidence hierarchy’ illustrates the
strength of the various types of
evidence (Figure 2), which
includes evidence from expert
opinion, non-experimental studies
such as qualitative and cohort
studies, experimental investigations,
including quasi-experimental
studies, randomised controlled trials
(RCTs) and systematic reviews of
RCTs (Borgerson, 2009; LoBiondo-
Wood and Haber, 2010).
LEVELS OF EVIDENCE
Various levels of evidence exist to
guide nurses. Generally, the higher
the level of the evidence, the less
likelihood of bias in the results and
the more rigorous the research.
Where higher level evidence
exists in wound care, this should
be included in evidence-based
treatment protocols.
Low-level evidence
These include expert opinions
formed through the researcher’s
experience and observations, as
well as case reports and case series
(Guyatt et al, 2008). Because these
kinds of evidence comprise reports
of cases but do not feature control
groups to compare outcomes, they
have little statistical validity. In the
absence of higher level evidence,
case studies and expert opinion
can be used by clinicians to
determine the best wound care
interventions, albeit with variable
patient outcomes.
Moderate-level evidence
Non-experimental studies are
regarded as more robust than expert
opinion and can include longitudinal
or cohort studies, which are typically
observational in nature but lack
any manipulation of variables, such
as wound type, duration, and size
(Dearholt and Dang, 2012). Cohort
studies are not as reliable as RCTs,
as the researchers observe without
an intervention and the group are
not matched, whereas in an RCT you
have an intervention for one group
of patients, but the patients in the
non-intervention group are matched
as in age, wound type, etc. However,
cohort studies can complement
RCTs in that it is helpful to look at
what is happening in real life.
High-level evidence
The two types of evidence
considered to be the most valid
are systematic reviews and RCTs
(Roecher, 2012). RCTs are carefully
planned experiments that introduce
a treatment, as in a type of dressing
or bandage, to study its effect on real
patients. They include methodologies
that reduce the potential for bias
(randomisation and blinding) and
allow for comparison between
intervention groups and control, or
non-intervention groups. An RCT
is a planned experiment and can
provide sound evidence of cause and
effect, but they can take considerable
time and are costly.
Systematic reviews focus on
a clinical topic and answer a
specific question. An extensive
literature search is conducted to
identify studies that have a sound
methodology. The studies are
reviewed, assessed for quality, and
the results summarised according
to the predetermined criteria of the
review question. A meta-analysis
will thoroughly examine the studies
identified in the literature search
and mathematically combine the
results using an accepted statistical
methodology to report the results
(Dissemond et al, 2017).
i
Practice point
The higher the level of evidence,
the more robust the findings and the
more relevant to the patient group.
Figure 1.
Components of evidence-based care (EBP=evidence-based practice).
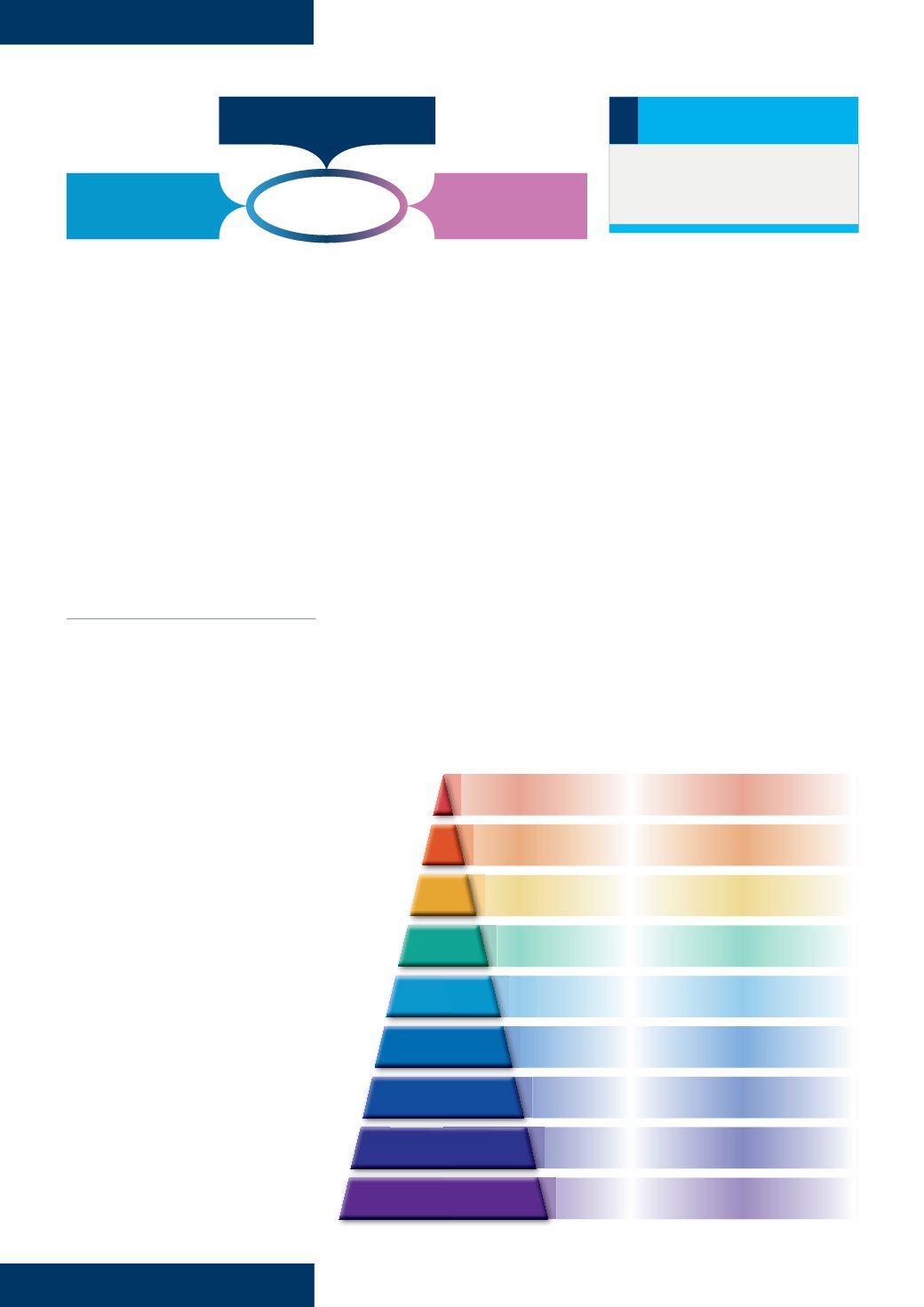
Figure 2.
Hierarchy of evidence.
Clinical expertise
Best research
evidence
EBP
Patient values and
preferences
1
2
3
4
5
6
7
Double-blind randomised controlled trials
Meta-analysis and systematic reviews
Randomised controlled trials
Non-comparative clinical trials
Cohort studies
Case series or studies
Individual case reports
8
Animal research,
in-vitro
studies
9
Best practice statements, consensus panels,
expert opinion