





 10 / 20
10 / 20

10 JCN
2015
JCN Roadshow
Asking this type of question will
help nurses decide whether or not to
debride, and by which method.
DRESSING/DEVICE SELECTION
The particular debridement technique
chosen will depend on a number of
variables, including:
Patient need: does he or
she have a wound that
needs debriding quickly
(with mechanical or sharp
debridement); or if the patient
is not fit for surgery or refuses
larval therapy for example,
could a slower method such as
autolytic debridement be used
(Gray et al, 2011)?
Nurse skill/competency: does the
nurse have the necessary skills to
perform debridement or will he or
she need to refer on?
The organisation’s formulary:
what products are available?
Which type of debridement?
The type of debridement used will
depend on many factors including:
Skill: do nurses have the skill
to use sharp debridement, for
instance, or will they need to use a
slower method such as autolysis?
Resources: for example, is there
nursing time available for autolytic
debridement, which can involve
multiple dressing changes?
Cost and effect: is the proposed
method of debridement the
most cost-effective, i.e. will a
one-off session of mechanical
debridement be cheaper than a
(see below for the use of Debrisoft
®
[Activa Healthcare]).
The fact that autolytic
debridement can involve numerous
dressing changes as the necrotic
tissue softens and is absorbed into
the dressing, also means that it can
be costly in terms of the amount of
dressings used and nursing time.
Autolytic debridement is also
associated with anaerobic odour
(produced as the tissue is slowly
broken down), as well as maceration
of the surrounding skin (caused by
the increase in moisture resulting
from softening tissue).
Larval therapy
This debridement technique involves
larvae being applied to the wound
either in a sealed mesh bag, or ‘free-
range’. The larvae secrete an enzyme
that semi-liquefies the necrotic tissue,
thereby allowing it to be ingested.
For a number of reasons larval
therapy is not a technique that is
suitable for all patients, for example:
The position of the wound may
make it difficult to apply the
maggots — if applied to sacral
wounds for example, the person
may crush the maggots when
sitting or lying down
Dry wounds with hard eschar that
may not liquefy.
Larval therapy is a skilled
method of debridement, but it
can be applied by nurses who
have received specialist training.
It is also important to balance the
fact that larval therapy may be
more expensive than some other
debridement methods, but involves a
shorter treatment period.
Mechanical
Although rarely used in the UK now,
the so-called ‘wet-to-dry’ technique
was once a popular debridement
method and involved using a
dressing to ‘dry-out’ the top layer of
the wound, which adhered to the
dressing. This top layer of the wound
then ‘came away’when the dressing
was subsequently removed. Not
only was this method potentially
painful and traumatic, it was also
non-selective, removing healthy and
unhealthy tissue.
programme of larval therapy?
Frequency: how often is
debridement required, e.g. as a
one-off session of mechanical/
sharp debridement; or as a
longer programme of autolytic
debridement?
Types of debridement
The most common methods of
debridement are:
Autolytic
Larval
Mechanical
Hydrosurgical
Ultrasound
Sharp
Surgical.
Autolytic
Autolytic debridement is effectively
the use of the body’s own enzymes
to soften and eventually remove
devitalised tissue. This is done by
covering the wound with a dressing
that promotes a moist wound-healing
environment, usually a hydrogel,
hydrofiber or hydrocolloid.
As highlighted in this session, the
main benefits of autolytic debridement
are that there is little pain involved
and it is a versatile and easy technique
with nurses being easily trained in
how to apply dressings and check for
the softening of necrotic tissue.
Autolytic debridement is also a
useful technique to soften devitalised
tissue in preparation for the use of
larvae or mechanical debridement with
a monofilament fibre debridement pad
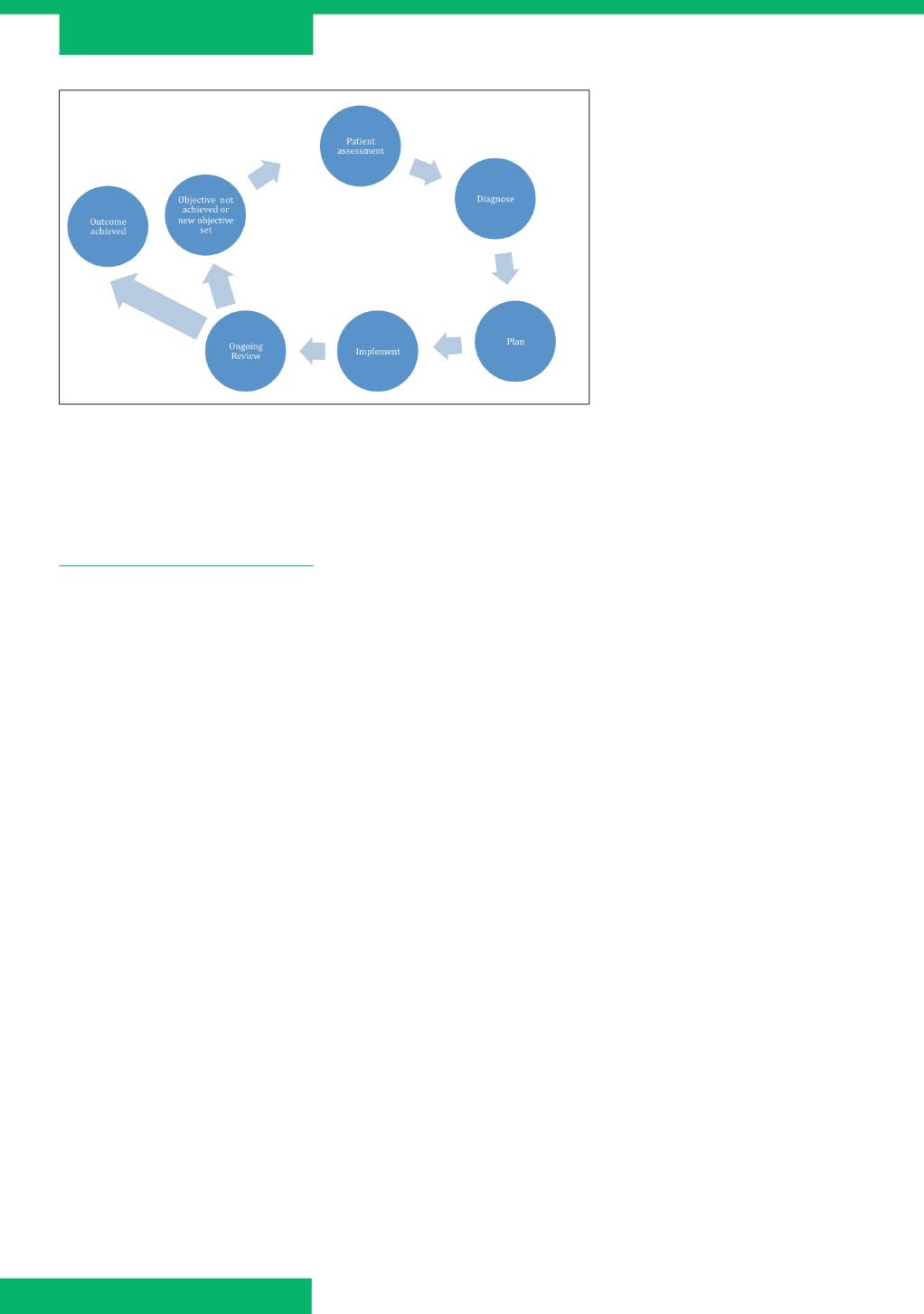
Figure 2.
A structured approach to assessment, diagnosis and management is vital in
any type of wound (Gray et al, 2011).