







 6 / 20
6 / 20

COMMUNITY WOUND CARE
6
JCN supplement
2015,Vol 29 No 5
Each patient’s wound is affected
by physical and psychological
elements, as well as social factors.
Previously diagnosed health issues
such as diabetes are known to mask
problems such as wound infection.
The patient must be supported
to maintain their diabetes at the
optimum level to gain the positive
effects of wound healing (European
Wound Management Association
[EWMA], 2008).
The negative effects of smoking
on general health have been well-
documented in the past (Silverstein,
1992), specifically in wound healing.
As well as referral to mental
health services, these patients need
supportive wound care and advice
as to how to prevent or manage any
infections. Ousey and Ousey (2010)
have reminded practitioners that
those patients who self-harm must
have a holistic wound assessment
that includes questions about their
preferred treatments. It may be that
patients will continue to delay wound
healing, however if they are supported
by the whole healthcare team, long-
term harm may be avoided.
CHRONIC WOUND CARE
Where wounds have become
senescent and are failing to heal,
admission to a community hospital
allows for the wound to be re-
assessed and a differential diagnosis
made. Drew et al (2007) suggested
that up to one-in-three chronic
wounds remained unhealed for at
least six months, and one-in-five
for a year or more. This is not to say
that district nurses are unable to
manage patients’wounds effectively;
rather that placing patients in a
more appropriate care setting means
procedures can be undertaken
more efficiently.
Chronic wounds can lead to:
`
Increased risk of infection
`
Psychological stress
`
Impaired skin function
`
Odour
`
Reduced nutritional status
`
Sub-optimal clinical and
cosmetic outcome.
Cavity wounds
Cavity wounds are a common type
of chronic wound that often develop
as a result of pressure ulcers, diabetic
Nicotine is a vasoconstrictor that
reduces the nutritional blood flow to
the wound and surrounding tissues,
resulting in ischaemia and impaired
healing. Patients who smoke can
be offered alternatives to nicotine
and referral to smoking cessation
specialists while in hospital.
Wounds need nourishment to
heal and older patients may have
difficulty maintaining the adequate
dietary intake required. Timms
(2011) advised early identification
of patients at risk of poor nutrition
and referral to dietitians. While it is
important that patients’ nutritional
needs are assessed while they are
still in hospital, it is also necessary
to consider how sufficient nutrition
will be provided on discharge.
In some cases, patients may
inflict their own wounds. Known
as factitious wounds, these injuries
can be unusual in presentation and
fail to heal whatever treatment is
used. Self-harming is a behaviour
not an illness, and the cause of the
patient’s distress will need to be
investigated by the mental health
team. Self-harm is a problem that
is being increasingly recognised
in ex-military personnel and
unfortunately the UK has the
highest numbers of people across
Europe that self-harm (Royal
College Psychiatrists, 2010).
To a degree, a ‘non compliant’
older person with a long-term leg
ulcer might be considered to be
self-harming if they continued to
sabotage treatment to retain a level
of communication with healthcare
staff, for instance.
Careful monitoring of the
patient’s environment may indicate
how the wound was inflicted.
Various techniques can be used to
either create a wound or ensure
that it remains open. In the author’s
clinical experience, these can
include washing wounds in bleach
(this presents as highly excoriated
and painful periwound skin) and
even setting fire to the bandages/
dressings. Scissors, razor blades,
pens and cigarettes have also been
used as ways of maintaining a
wound (Corser and Ebanks, 2004).
i
Practice point
:RXQGV QHHG QRXULVKPHQW WR
KHDO DQG ROGHU SDWLHQWV PD\
KDYH GLIÀFXOW\ PDLQWDLQLQJ WKH
DGHTXDWH GLHWDU\ LQWDNH UHTXLUHG
(DUO\ LGHQWLÀFDWLRQ RI SDWLHQWV DW
ULVN RI SRRU QXWULWLRQ DQG UHIHUUDO
WR GLHWLWLDQV LV LPSRUWDQW :KLOH
LW LV LPSRUWDQW WKDW SDWLHQWV·
QXWULWLRQDO QHHGV DUH DVVHVVHG
ZKLOH WKH\ DUH VWLOO LQ KRVSLWDO
LW DOVR QHFHVVDU\ WR FRQVLGHU
KRZ VXIÀFLHQW QXWULWLRQ ZLOO EH
SURYLGHG RQ GLVFKDUJH
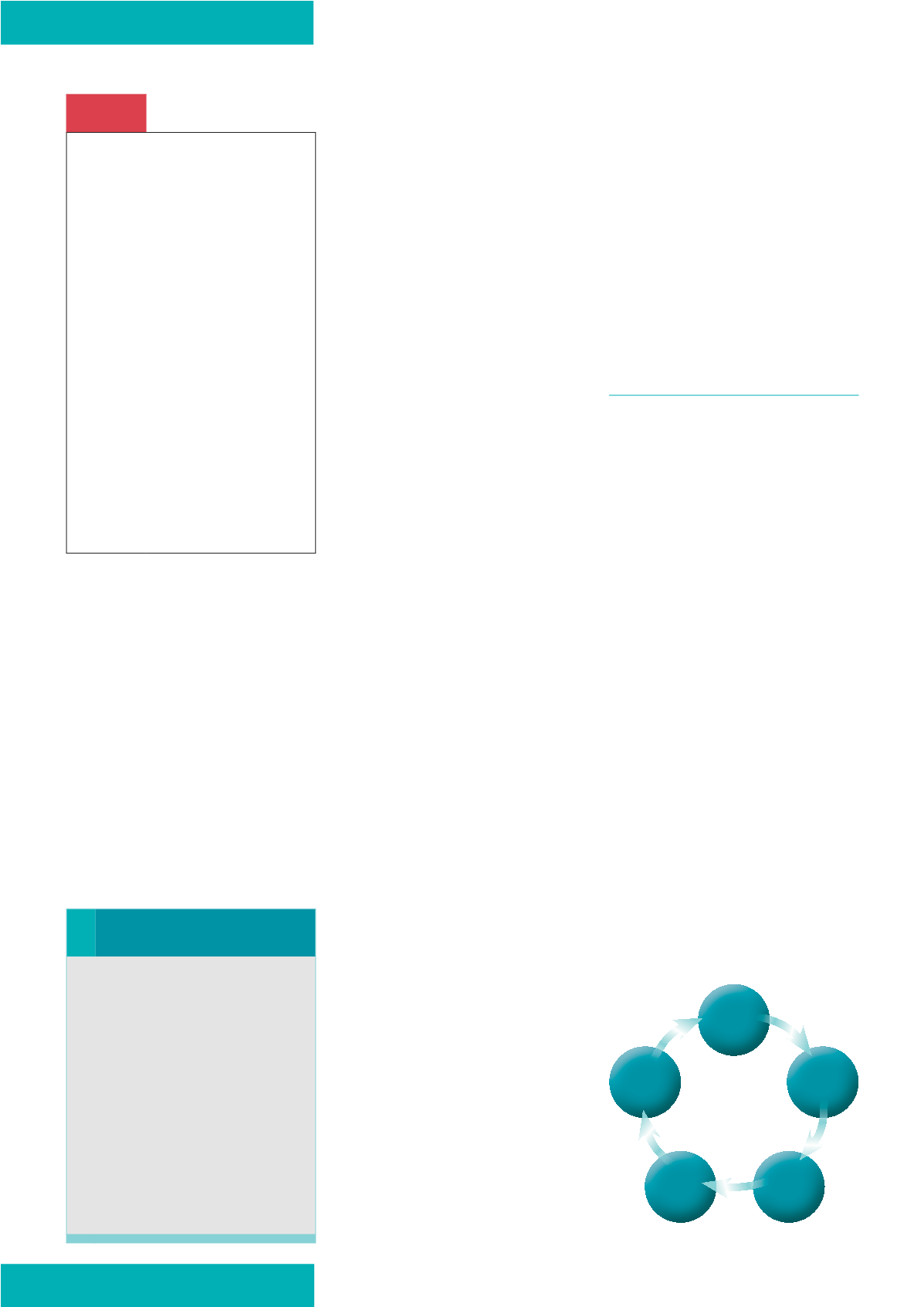
Figure 2.
A typical pathway of care.
Red Flag
Infection
:RXQG LQIHFWLRQ UHVXOWV IURP
WKH LQDELOLW\ RI WKH SDWLHQW·V
ERG\ WR FRQWURO WKH EXUGHQ
RI EDFWHULD ZLWKLQ D ZRXQG
,GHQWLI\LQJ WKRVH IDFWRUV ZKLFK
LQFUHDVH WKH OLNHOLKRRG RI
LQIHFWLRQ DQG PD[LPLVLQJ WKH
SDWLHQW·V QDWXUDO GHIHQFHV DUH
HVVHQWLDO VWHSV LQ SUHYHQWLQJ
LQIHFWLRQ ,I LQIHFWLRQ RFFXUV LW
LV LPSRUWDQW WKDW FOLQLFLDQV DUH
DEOH WR LGHQWLI\ WKH VLJQV DQG
V\PSWRPV DQG LQLWLDWH VSHHG\
DQG DSSURSULDWH WUHDWPHQW
-XGLFLRXV XVH RI WRSLFDO
DQWLPLFURELDO ZRXQG GUHVVLQJV
KDV SURYHQ WR EH DQ HIIHFWLYH
PHWKRG RI UHGXFLQJ ELREXUGHQ
DQG HQDEOHV FOLQLFLDQV WR UHVHUYH
WKH XVH RI DQWLELRWLFV IRU WKRVH
SDWLHQWV LQ JUHDWHVW QHHG
History
Investigation
Diagnosis
Indicators
(for progress)
Examination