





 32 / 56
32 / 56

32
WOUND CARE TODAY
2017,Vol 4, No 1
FOCUS ON
M
OISTURE
i
Top tip:
Exudate is a good indicator of the
state of a wound. Changes in colour,
amount, viscosity or smell can be a
trigger to reassess the wound.
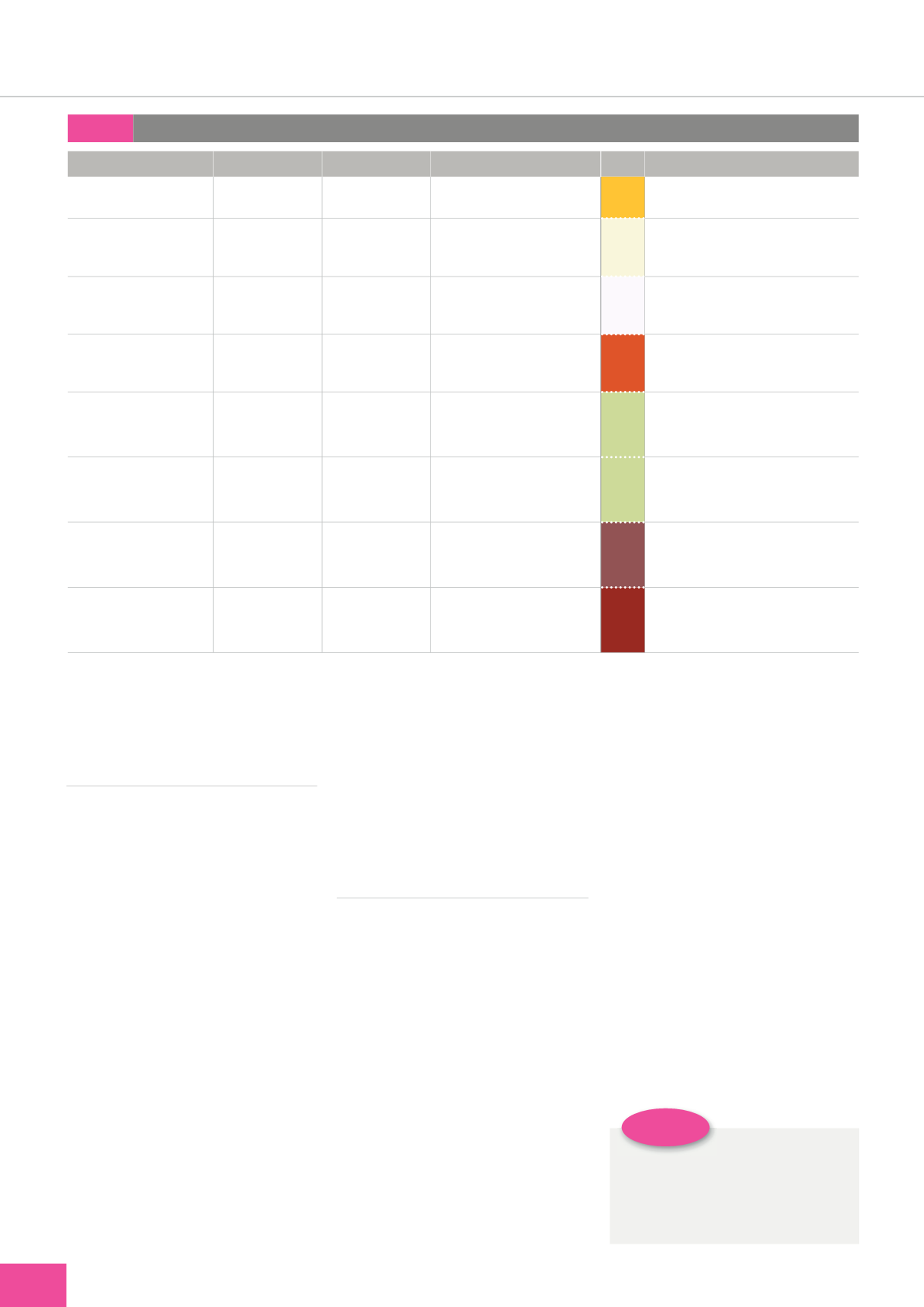
Table 1:
Exudate assessment (adapted with permission from Cutting, 2004)
Underlying cause
Type
Volume
Description
Interpretation
Acute injury to superficial
or partial-thickness wounds
i
Serous
i
Low–moderate
i
Clear, thin, watery, amber-
coloured exudate
i
Inflammatory exudate normal
within the first five days of acute injury
Acute injury with presence
of bacteria or superficial
non-viable tissue
i
Fibrinous
i
Low-high
i
Creamy, cloudy, thin
exudate with the presence of
fibrin protein strands
i
Inflammation or local infection
Acute injury, post
operatively or trauma on
dressing removal
i
Serosanguinous
i
Low–moderate
i
Clear, watery, thin, pink-
coloured exudate
i
Inflammatory exudate with mild
capillary damage
Acute injury, post
operatively or trauma on
dressing removal
i
Sanguinous
i
Low–moderate
i
Watery, thin, red-coloured
exudate
i
Trauma to blood vessels
Chronic wound with non-
viable tissue present
i
Seropurulent
i
Moderate–high
i
Yellow/grey/green, thick
exudate
i
Local or possibly
spreading infection.
Liquefaction of
necrotic sloughy tissue
Acute wound dehiscence or
chronic wound with non-
viable tissue
i
Purulent
i
Moderate–high
i
Yellow/grey/green, thick
exudate
i
Indicative of bacterial infection, e.g.
Pseudomonas aeruginosa
Acute wound dehiscence or
chronic wound with non-
viable tissue
i
Haemopurulent
i
Moderate–high
i
Viscous, thick, sticky red/
brown exudate
i
Confirmed spreading infection
Acute deep wound trauma
or chronic wound with
extensive non-viable tissue
i
Haemorrhagic
i
High
i
Thick, dark red exudate
i
Vessel damage from trauma or
chronic wound infection. Capillaries
are friable and spontaneously bleed
tissue, a large volume of bacteria in
the wound and malodour (Wounds
UK, 2013).
NEGATIVE IMPACT
OF WOUND EXUDATE
The presence of wound exudate can
be the most distressing aspect of
having a wound for an individual
and their carers. The impact of
copious exudate and odour on the
individual’s quality of life in many
cases is intolerable, and empirical
evidence demonstrates heightened
anxiety, depression, embarrassment
and social isolation in patients with
wet, malodorous wounds (Franks
et al, 2003; Eagle, 2009; Meaume et
al, 2017). Tissue damage resulting
from exposure to exudate, such as
maceration and excoriation (see
practice point boxes
) causes pain,
discomfort and delayed healing
(Whitehead et al, 2017).
In addition to the negative
impact on patient quality of life,
exudate can result in significant
expense as a result of attempts
to mask odours and contain the
fluid. Protective sheets and towels,
replacement bedding, footwear or
clothing and increased washing
may be necessary where exudate
is uncontrolled, which is time-
consuming and distressing for
patients and carers. And, indeed,
can be challenging for those
patients who are physically less able
(Tickle, 2016).
LOCAL WOUND ASSESSMENT
Moisture is required by the wound
throughout the wound healing
process. It promotes the natural
autolysis of devitalised tissue in
the destructive phase of healing
and enhances epithelialisation
in the latter stages (Dowsett and
Newton, 2005). However, there is a
subtle balance between the wound
bed being too wet or too dry; a
dry wound will have reduced cell
proliferation, while a wet wound
will have non-viable macerated
cells preventing epithelialisation
from the wound edge (Myers, 2012).
Both sets of conditions will result in
delayed healing which increases the
risk of local and systemic infection.
While acute wound exudate
is a normal response within the
inflammatory stage of healing,
chronic wound exudate is either
a symptom of a local problem
with the wound, such as critical
colonisation, biofilm formation or
infection, and/or results from an
underlying condition such as venous
disease, oedema, hypoalbuminaemia
or organ failure.
Establishing why the wound
is producing copious exudate is a
prerequisite to establishing effective
treatment goals for the individual.
Consequently, as part of holistic
wound assessment, the volume,
colour, consistency and odour of
exudate should be evaluated and
recorded, along with its effects, if
any, on the skin surrounding the
wound (WUWHS, 2007)(
Table 1
).