44
WOUND CARE TODAY
2015,Vol 2, No 1
FOCUS ON MOISTURE LESIONS
›
Reassessment needs to take
place regularly every 24–48 hours,
and sometimes more frequently
depending on the severity of the
skin damage and the patient’s
environment. For example, those
in hospitals and care homes will
have 24-hour access to staff, making
observations easier than for those at
home. This is particularly important
in patients with incontinence and any
skin changes must be documented
and a robust plan to protect the skin
put in place.
MANAGEMENT
Incontinence
A key factor in the prevention of
moisture lesions is the accurate
assessment and management of
incontinence. If the cause of the
incontinence cannot be treated, a
variety of continence products are
available, including:
›
Body-worn incontinence pads
›
Urinary sheaths and
containment devices
›
Urinary catheters
›
Urinals and absorbent gels
›
Anal plugs
›
Faecal collectors
›
Faecal management systems.
Each patient should be
individually assessed to ascertain
the best product for his or her needs.
This should be reassessed regularly to
ensure the product remains the most
appropriate.
Nutrition
Effective management of the
nutritional status of the patient can
improve the strength of the skin and
reduce the risk of skin breakdown.
Encourage the patient to drink
enough to maintain good hydration
as this will also dilute the urine
(concentrated urine has an increased
amount of waste products and a
higher pH and can be detrimental to
the skin).
A nutritional assessment should
be carried out in those patients who
already have moisture lesions as well
as those thought to be at risk.
Skin care
A good skin care regimen is very
important and should be performed
immediately after soiled and wet skin
has been cleaned. It is also important
to avoid the over-hydration that
can be caused by excessive washing
(Ersser et al, 2005).
The skin should be cleansed
following each episode of
incontinence with a low pH soap
and warm water. Normal soap can
dehydrate the skin and contains
surfactants that can irritate the skin,
which can make it more susceptible
to breakdown (Bale et al, 2004).
like the ‘perirectal skin assessment
tool’ (Storer-Brown, 1993) considers
specific areas in the sacral/buttock
area. The latter is the easiest tool to
use as it splits the excoriation into
mild, moderate, and severe, and has
pictures to aid the clinician.
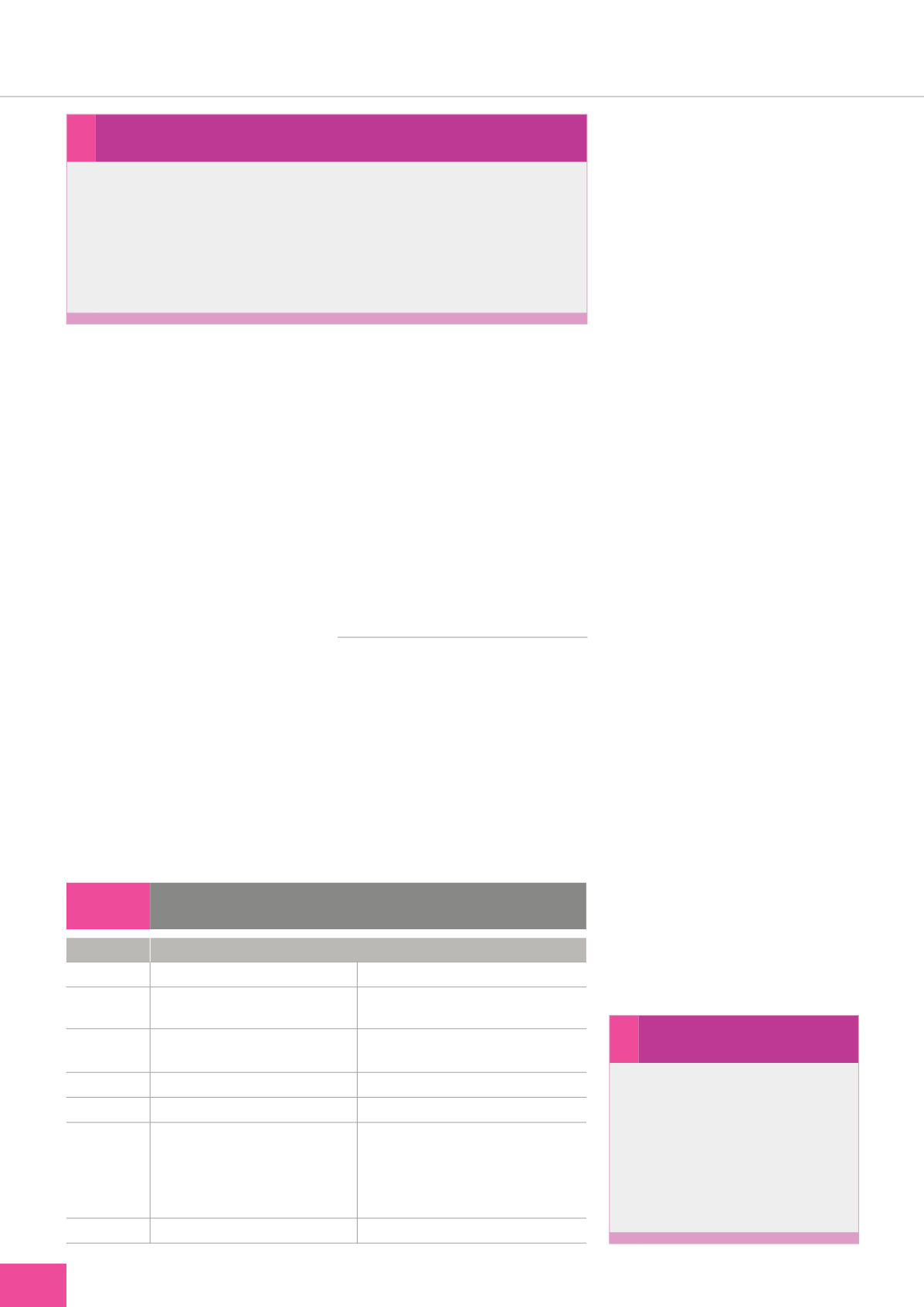
There are clear differences
between moisture lesions and
pressure ulcers and by working
through these differences it enables
the practitioner to establish the
correct diagnosis (
Table 1
).
Holistic assessment
An holistic assessment of the
patient should include an accurate
skin assessment with particular
attention paid to the perianal area,
natal cleft, and between the thighs,
buttocks and scrotum/labia, as
all these areas can be affected by
moisture lesions.
In severe cases, the erythema may
extend to the lower abdomen and
sacrum (Beldon, 2008).
›
Wound facts...
Uncontrolled diarrhoea can cause
dehydration, gradually draining
the body of the fluids it needs to
function properly. Dehydration is
particularly dangerous in children
and older people, and must be
treated quickly to avoid serious
health complications.
Table 1:
Differences between moisture lesions and pressure ulcers (Evans and
Stephen-Haynes, 2007)
Moisture lesion
Pressure ulcer
Cause
›
Moisture
›
Pressure and/or shear and friction
Location
›
Natal cleft or on the wider buttock
not over a bony prominence
›
Over bony prominence
Shape
›
Mirror image, linear in shape
›
Diffuse in several superficial spots
›
Takes on shape of the causative pressure,
often limited to one spot
Depth
›
Superficial
›
Superficial or deep
Edges
›
Diffuse or irregular edges
›
Distinct edges
Colour
›
Non-uniform redness
›
Blanchable or non-blanchable
erythema
›
Pink or white surrounding skin due
to maceration
›
Uniform redness
Necrosis
›
No necrosis
›
Necrosis can be present
›
Incontinence and the skin...
The normal pH of the skin is between 4.5 and 6.2. To keep the skin
intact it is essential to maintain the acidic pH of the skin. With
incontinence, ammonia is produced as a result of the breakdown of
urinary urea and aggravated by faecal urease, resulting in an increase
in the pH of the skin. The skin becomes more permeable when the
pH rises, which is exacerbated by excessive moisture and eventually
causes invisible breaches on the skin’s surface.


