Granulox
®
haemoglobin spray
7
Case report
6
This 60-year-old female patient
had undergone an emergency
sternotomy six years previously.
Due to her recurrent ill-health
— including a history of cardio-
pulmonary respiratory disease
(COPD), hypertension, myocardial
infarction and tracheostomy — the
wound had undergone several
episodes of infection, which required
intravenous antibiotics. The sternal
wound had now dehisced and was
not responding to treatment with
antimicrobial dressings containing
both honey and silver. The wound
had significantly disrupted the
patient’s quality of life and her
dressings were being changed daily
by district nurses to address the
odour and excess exudate, which
prevented her from socialising.
Despite alternating between honey
and silver dressings, the district
nurses were unable to achieve
healing — the exudate was not
being contained and the tissue in
the wound bed had a thick, dull
and yellow appearance. It was
also malodorous.
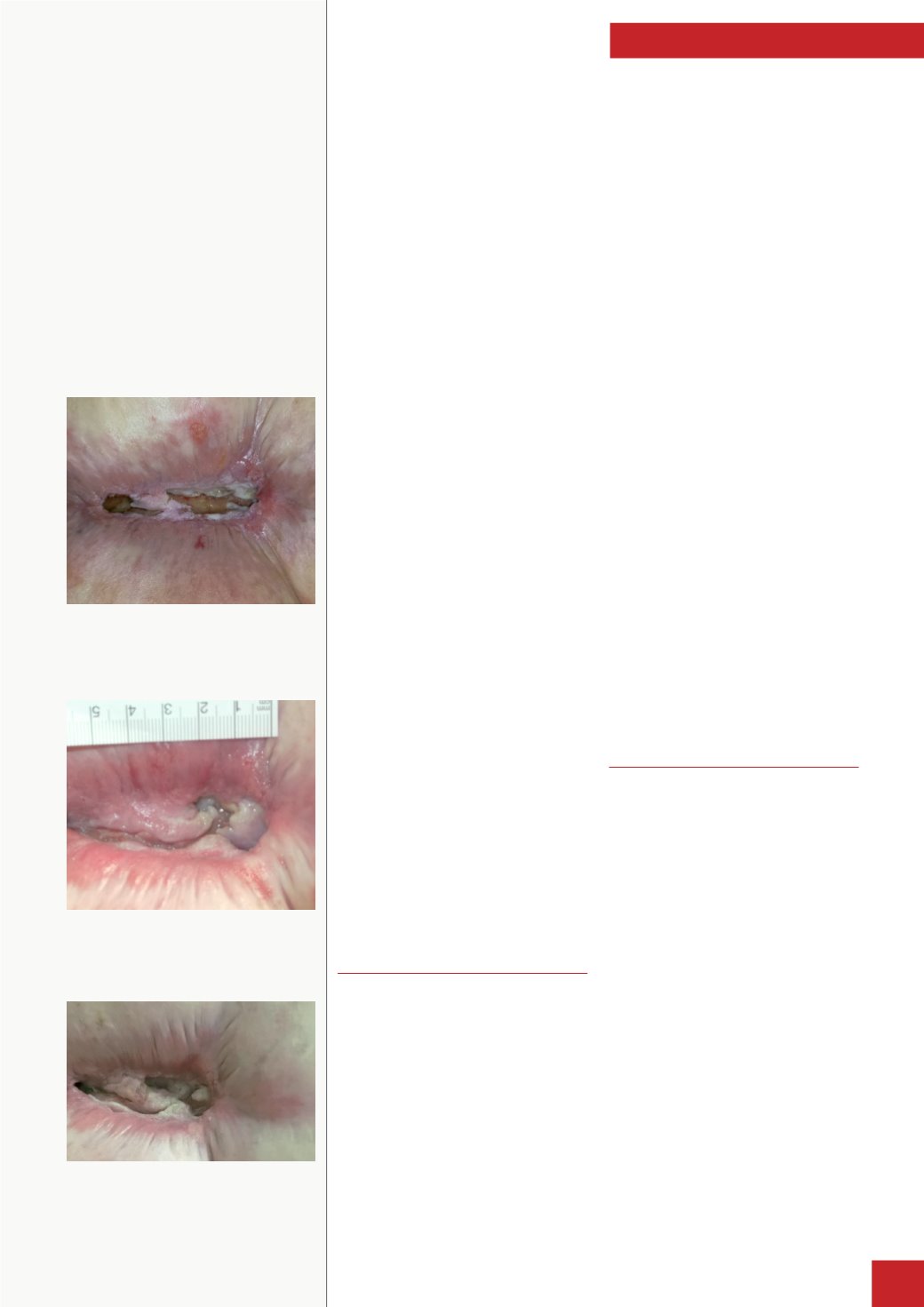
When the patient was referred to
the author the wound measured
9x5x1.5cm (
Figure 1
). The wound
bed was ‘stagnant’ and comprised
100% sloughy tissue, with cloudy,
highly viscous exudate. The
sternal bone was also visible. The
wound was critically colonised
and the surrounding skin was
red, macerated and excoriated.
The patient stated that she was
experiencing significant pain
(scoring it ‘8’ on a scale of 1–10, with
10 being the worst pain).
Starting on Granulox
®
The author began daily treatment
with a haemoglobin spray-on solution
(Granulox
®
). This product was chosen
because the wound bed showed little
sign of adequate oxygenation despite
the previous attempts to remove
biofilm. Granulox was applied directly
to the wound bed after it had been
soaked for five minutes in Prontosan
®
(B Braun) solution, then the previously
used antimicrobial dressing was
applied. The secondary dressing was
reassessed in an attempt to contain
the exudate more effectively, and it
was decided to use a foam dressing.
At a review of the wound at week
three of treatment, the author found
that there was no malodour and the
patient reported that the dressing
was staying drier for longer periods
of time. The wound size had reduced
to 7.5x2x0.5cm, and the tissue type
appeared healthier than it had two
weeks previously. Even though the
wound was still critically colonised,
the wound bed exhibited only
50% slough, with the other 50%
comprising red granulation tissue.
The periwound skin was still red, but
was no longer macerated. Crucially
for the patient, the exudate was now
thinner, there was no malodour and
her pain score had reduced to ‘5’.
At week eight of treatment with
Granulox, the wound was reassessed
and now exhibited 100% granulation
tissue. The size of the wound
had also reduced to 6x1.5x0.2cm,
and while not completely healed,
there was no evidence of critical
colonisation. Similarly, the
periwound skin had also improved
and the exudate production was now
only medium and clear-coloured.
There was still no odour and the
pain score had reduced to ‘1’.
Impact on patient
quality of life
Significantly, the patient’s quality
of life had vastly improved — she
stated that she could now ‘dress
up’ to go out without feeling
embarrassed or anxious about
odour or exudate. She also found
it easier to go about her everyday
business as the district nurses now
only needed to visit twice-weekly
for dressing changes and she had
even been away with her family for
an entire week.
From the author’s clinical
perspective, the wound size
and exudate production were
significantly reduced in the
treatment time and this had cost
implications as fewer district nurse
visits were required. Importantly,
the patient’s quality of life was
significantly improved.
Figure 2.
Wound at 29 April, 2014 showing
reduced slough and converging edges.
Figure 3.
Wound on 25 June, 2014 demonstrating
much-reduced size and improvements to
periwound skin.
Figure 1.
Sternal wound showing extensive slough
and macerated periwound skin.
This case shows how a dehisced sternal
wound that was not responding
to treatment with antimicrobial
dressings, progressed to healing after
eight weeks’ treatment with Granulox.
Granulox also improved activities
of daily living, as previously, odour
and excess exudate had prevented the
patient from socialising.


